Melanie Potock, MA, CCC-SLP and Amy Graham, MA, CCC-SLP show us how to do an oral-facial exam with Throat Scope.
Never miss a blog!
Subscribe to get updates on new blogs from Throat Scope.

Melanie Potock, MA, CCC-SLP and Amy Graham, MA, CCC-SLP show us how to do an oral-facial exam with Throat Scope.
Subscribe to get updates on new blogs from Throat Scope.
Surgeons and oncologists who work in Head and Neck Cancer Multidisciplinary Teams (MDTs) are qualified to do head and neck cancer screening. The process involves asking about possible symptoms, examining the mouth and the top of the throat with a good light source, and palpating the neck for lumps. Screening clinics which run outside traditional hospital environments are a great way to raise awareness of the signs and symptoms of these cancers, especially among people who may never have heard of the disease. Head and neck cancer screening also has one big advantage over many over screening clinics – we can examine the vast majority of patients without asking them to remove any items of clothing. In this blog I am sharing how we ran our screening clinic and what we learned in the hope that I can inspire other clinicians to do the same.
The goal for our head and neck cancer screening clinic was to raise awareness. My practice team had been brainstorming ideas for activities for World Head and Neck Cancer Day (WHNCD) to help bring attention to these diseases. Not only do most people know very little about head and neck cancer but also the majority of those who have heard about it are under the false impression that the main contributing lifestyle factor is smoking. We were aware of other head and neck cancer screening clinics being run in hospitals which recruited volunteer patients who consisted mostly of hospital staff, visitors and some members of the public. We wanted to stage an event that was held off a hospital campus in order to engage with a broader cross section of the general public. The date for WHNCD is July 27 which meant that in 2019 WHNCD fell on a Saturday. Sports fields and shopping centres seemed like good options and we knew we wanted the screenings to be free. We had plenty of ideas but the difficulty was putting them into action.
Fortunately for us we have been working for some time with Jennifer Holland and the team at Holland Healthcare. Jennifer is the inventor of Throat Scope, a tongue depressor with a light in it. Otolaryngology Head and Neck Surgeons (ENTs) routinely use specially designed light sources wen examining the mouth and throat. Not every doctor or clinician has access to this equipment. Throat Scope is a fantastic tool which enables GPs, dentists and other clinicians who regularly examine the mouth to complete a thorough oral examination without the need for a separate light source. Jennifer and her team had previously run an oral screening event in 2017 at the V8 Super Cars Newcastle. She offered to use her contacts to help us find a suitable venue to run our screening clinic on World Head and Neck Cancer Day. Jennifer did not disappoint and secured a spot for us at Bankwest Stadium among the pre-game activity during the National Rugby League premiership season when the Parramatta Eels played the New Zealand Warriors. We were stationed outside the main entrance. Thousands of people had to walk past our marquee to enter the stadium.
Before giving the project the green light we also approached Anthony Schembri AM, CEO of St Vincent’s Sydney and Dr Julia Maclean, president of the Australian New Zealand Head and Neck Cancer Society for their support. All clinicians participating in the event are members of both the St Vincent’s Head and Neck Cancer MDT and the ANZHNCS so it made sense to approach these organisations. St Vincent’s Sydney not only provided in principle support but also worked with me to create a video about neck lumps, one of the major symptoms of head and neck cancer, to run on St Vincent’s TV across their website and social media platforms on WHNCD.

In order to run our free screening clinic we needed the following personnel;

One major advantage of screening for head and neck cancer over screening for cancers on other sites of the body is that very few items of clothing need to be removed. That said, I admired a lot of Parramatta Eels beanies and scarves. But we still wanted to provide privacy to patients and created individual screening booths. In addition to a weather proof marquee, examination equipment and furniture we also needed banners, signage and patient literature. The banners and signs communicated what we were doing and the literature ensured people understood the screening process, the signs and symptoms of head and neck cancer, and where to find more information. Jennifer had the great idea of putting this information in the form of a postcard which included a link to the excellent online Head and Neck Cancer resources at the NSW Cancer Council


Each clinician worked in a screened consultation area within the marquee.

Literature needs to be easy to read and provide links to authority sources.
Running a pop up screening clinic is not risk free for patients, organisers or clinicians. We took advice from Avant Risk Management to ensure we understood what we were getting ourselves into. Patients who see clinicians at a free screening clinic like ours have the right to expect the same standard of care as they would if they were seeing the clinician at a pre-arranged appointment in a practice or hospital setting. We had to collect patient data, display a privacy policy explaining what would happen to that data, record the findings for each patient, and provide a letter for patients with an underlying suspected diagnosis to take to their regular GP for follow up. We only screened people over eighteen years of age. There was no power supply to our marquee so all of this had to be done by hand with pre-printed paper templates. Over the next few days my staff will enter all patient details into our patient database, scan and link records of each consultation to create a medical record, and follow up patients with a suspected underlying diagnosis to ensure they get the care they need. Medical records from the event will be retained in digital format in our secure system for the next seven years in accordance with medical record storage regulations and the paper versions will be appropriately destroyed in order to protect patient privacy. The staff at Bankwest Stadium were a pleasure to liaise with and made sure we met our responsibilities of providing a certificate of currency for public liability and that our marquee was weighted securely in case of severe wind gusts. We were very lucky with the weather, it was a spectacular winter’s day. We also had to remove our own rubbish and follow explicit set up instructions regarding access.
We screened just over one hundred patients in two and a half hours, including the Parramatta Eels cheer squad, Life Education Ambassador Healthy Harold, being a giraffe his neck examination took a little longer than average, and three fine members of the NSW Police Force. There was no shortage of patients. The Parramatta Eels supporters were out in force with over 17,000 people attending the game. We identified four patients with suspected underlying diagnoses, 4% of our patient cohort. The findings included enlarged lymph nodes in the neck and lip lesions. These patients were either unaware of their symptoms or unaware their symptoms required further investigation. Not surprisingly the group of Eels supporters smoking around the corner from us were reluctant to participate in the screening clinic. To their credit, they did take our literature and thanked us for the invitation.


Dr Julia completing a slightly tricky examination.

Police officers participating in screening after checking the 17,000 strong crowd was safely in the stadium.
Yes, this event was definitely a success, we achieved our goal of raising awareness of head and neck cancers, not just among the patients we examined but also among people with whom we had conversations and to whom we distributed printed information. I will also say that it was not just the patients who benefitted. My team and I had an exhausting but uplifting day getting out of our regular environment and talking to a huge range of people about these rare cancers. It was rewarding to reassure those patients who were scared of what we might find when they volunteered to be examined, and it was delightful to screen patients who were happy and relaxed, an unusual experience for someone like me who spends most days diagnosing cancer. Our findings of four patients requiring follow up confirms that we interacted with a general cross section of the population.
Definitely. We look forward to doing other free Head and Neck Cancer screening events in the future. In the public conversation about cancer neither head and neck cancer nor head and neck cancer patients receive the attention or funding they deserve. Taking direct action to screen one hundred people may sound like a drop in the ocean but the success of the event only strengthened me and my teams’ resolve to keep working to raise awareness. If clinicians like me don’t do it who will.

The entire head and neck cancer clinic screening team – three support members to every one clinician.
Hi Richard Gallagher’s my name and I’m a head and neck surgeon at St Vincent’s. I work at St Vincent’s Private Hospital, St Vincent’s Public Hospital, and at The Kinghorn Cancer Centre. I’ve worked at St Vincent’s since 1998. I finished my surgical training in 1995 and following that I did further training in head and neck cancer surgery. At the present time my practice is mainly looking after patients with cancer and head and neck cancer and looking after patients with complex airway problems. In 2011 I went and did further training in the United States in Philadelphia at the University of Pennsylvania in transoral robotic surgery. So that surgery’s used mainly for patients who havecancers at the back of the throat and oropharynx and is particularly useful for patients who have cancers due to the human papillomavirus or HPV. So that’s a large number of patients at the present time. On the campus I also wear several hats. I’m the Director of Cancer Services and I’m also the Director of the Head and Neck Cancer Service at St Vincent’s.
Subscribe to get updates on new blogs from Throat Scope.

April is Oral Cancer Awareness Month, when our attention turns once again to a cancer that continues to increase each year. It’s true that five-year survival rates have improved, but they aren’t getting better because of earlier discovery or innovative screening techniques. Instead, these rates correlate with the increase in HPV-related oral and, in particular, oropharyngeal cancers that are more sensitive to treatment modalities, elevating survival rates.
The collection of research data from the national cancer registries once predicted that by 2020, HPV-related oropharyngeal cancers would surpass HPV-related cervical cancers as the anatomical site with the highest burden of HPV-related cancers. Well, we have far surpassed this prediction. Again, based on data from national registries, HPV-related oropharyngeal cancer surpassed HPV-cervical cancer in 2015!

The biggest concern is that the majority of the North American population is unaware of the risk this very common virus presents. There is limited knowledge of the human papillomavirus being the culprit behind this escalation. How common is HPV? The Centers for Disease Control and Prevention (CDC) estimate that it is so common, almost every American adult will have an infection at some point in his or her lifetime.
For the majority of the population that has a normal functioning immune system, the virus will be cleared from the body often without awareness or recognition, similar to the common cold virus. For those who incur a persistent infection with a high-risk strain of the virus, such as HPV-16, there is an increased risk for transformation from an infection to malignancy.
The CDC further reports that HPV is believed to be the cause of 70% of oropharyngeal cancers in the United States. Smoking and alcohol historically have been the two most well-known etiologic pathways. Many of our patients feel that if they are non-smokers and non-drinkers, they won’t have an inherent risk for oral and/or oropharyngeal cancer. This mindset needs to be eliminated, and education needs to abound.
As a dental professional, our professional standards of practice require us to perform an extraoral and intraoral soft tissue examination, which includes an oral cancer screening, at least once a year on all adult patients. The oral cancer screening is not an option. It is our responsibility. Furthermore, educating our patients about the importance of self-examination at home and initiating a self-referral is a supportive and strong step toward earlier discovery. This was the impetus behind the launch of the North American “Check Your Mouth” campaign.
The North American launch of the public campaign has been a long awaited aspiration of the Oral Cancer Foundation and specifically of its founder, Brian Hill, a stage IV oral cancer survivor. Throat Scope, the world’s first all-in-one illuminated tongue depressor, is the ideal tool to facilitate effective self-examinations for the public campaign. The partnership between the Oral Cancer Foundation and Throat Scope has created an organically driven movement gaining momentum across North America.
Through education provided on the Check Your Mouth website, our patients will have an elevated awareness of what to look for and what shouldn’t be ignored, reinforcing the need for self-referral and examination by a dental professional. The hope and objective of the campaign is to eliminate the long period between regularly scheduled professional care and the opportunity for assessment of an abnormal finding.
This by no means detracts from the importance of regular professional oral cancer screenings. In fact, it reinforces their importance. The key to saving lives is the earliest possible discovery of something abnormal. When an oral lesion is discovered in the early or localized stage, five-year survival rates are impacted significantly, accompanied by an improved quality of life for survivors. Oral and oropharyngeal cancers are still found at later stages primarily due to a lack of public awareness and a lack of routine opportunistic screening programs being employed.
Providing our patients with five life-saving minutes in the form of a professional visual and tactile oral cancer screening examination is first and foremost the most important step to earlier discovery of an abnormal lesion. The next step is directing them to invest five life-saving minutes in performing a self-examination of their face and neck and inside their mouth on a monthly basis. It is through this familiarity that a new finding will be most readily recognizable. A persistent finding, being anything that does not resolve within two weeks, should be further examined by a dental professional.
The Check Your Mouth website provides an educational video illustrating a step by step self-examination of the face and neck and inside the oral cavity and visually accessible areas of the oropharynx. It also provides an overview of what to look for, complemented by a visual gallery of normal versus abnormal findings. The often subtle, lifesaving symptoms are outlined along with risk factors. The recommended tools are available for purchase through the website as well.
Together, we can make positive inroads in ensuring that we are doing our part to save lives and prevent the later-stage discovery of oral cancer.

Ms. Jones is an international award-winning speaker and was selected to join Dentistry Today’s Leaders in CE for the tenth consecutive year in 2020. She is also an Advisory Board Member for Holland Healthcare. While preparing to present her research on HPV-related oropharyngeal cancer to her national association, a family member received a diagnosis of late-stage HPV tonsillar cancer, succumbing to the disease 16 months later. Ms. Jones proudly partners with the Oral Cancer Foundation in conveying the urgent need for changing the way in which we screen for oral cancer to meet the needs of today’s population. She can be reached at via email at jjones@jo-annejones.com.
Disclosure: Jo-Anne Jones is a contributor to the project management team for the Check Your Mouth campaign. She also serves as an advisor to Throat Scope and is involved in the North American launch of Throat Scope into the dental community.
Read the original article HERE.
Subscribe to get updates on new blogs from Throat Scope.

I love simple ideas that are genius. Today’s post is a Throat Scope Review and it’s one of those simple genius ideas. You know, the kind that make you say, “Why didn’t I think of that?” A company from Australia, Holland Healthcare, reached out to me a few weeks ago and I was instantly interested in their product. Throat Scope is an illuminated tongue depressor. Wait, seriously, why didn’t I think of that?!

They sent me a Throat Scope and set of blades to test out and I am so impressed with this product. The simplified review? It works, reduces the materials I need, and engages kids. It’s a win.
Throat Scope was started by a company in Australia. It was actually featured on Shark Tank Australia.

 My brother was in town and I forced him to let me inspect his oral cavity using the throat scope. I was surprised at the amount of light the Throat Scope puts out. It definitely works!
My brother was in town and I forced him to let me inspect his oral cavity using the throat scope. I was surprised at the amount of light the Throat Scope puts out. It definitely works!
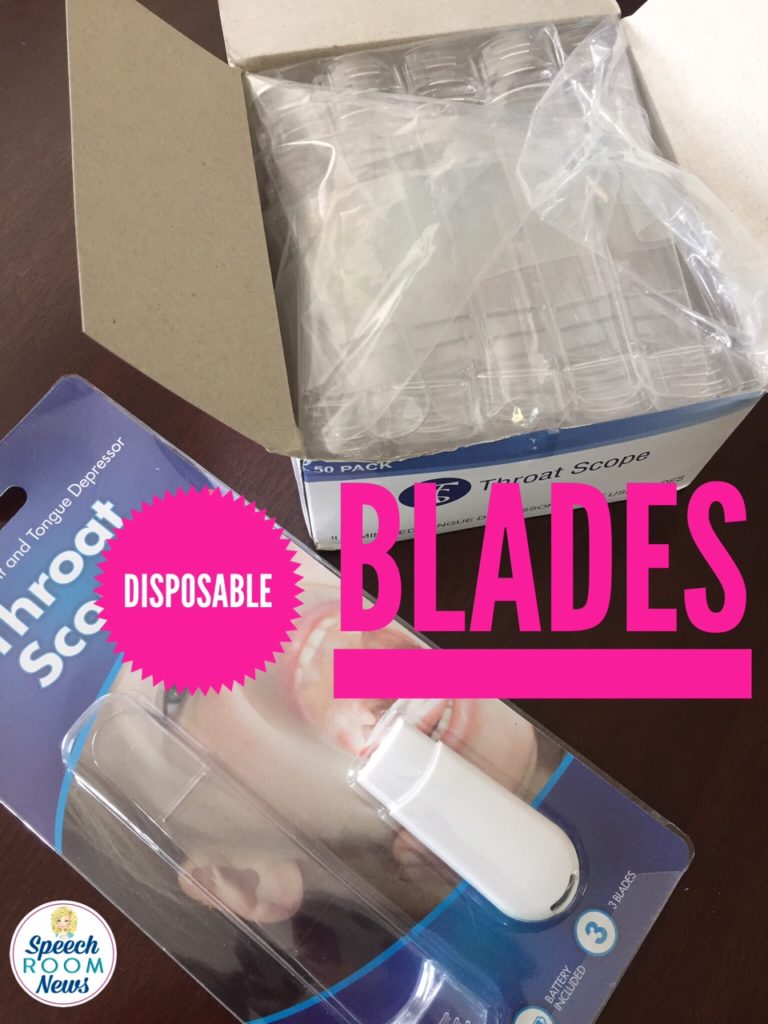
The disposable blades make it perfect for healthcare.
If you want more details about the Throat Scope, visit their website.
This product was provided for review, no other compensation was provided and these opinion belong to me! And that’s my Throat Scope review :)

Read the original blog by Jenna at The Speech Room News HERE.

My name is Jenna Rayburn Kirk, M.A.,CCC-SLP. I’m an ASHA certified pediatric speech-language pathologist. I work in the Columbus, Ohio area. I’m a graduate of The Ohio State University and Ohio University. My clinical experience has focused on pediatric speech and language therapy. I’ve worked with children aged 2-15 in schools and clinics. My current interest is in preschool-aged children. I work in a public school full-time in central Ohio.
Subscribe to get updates on new blogs from Throat Scope.

The Oral Cancer Foundation (OCF) has launched a new nationwide campaign aimed at the early self discovery of oral cancers. The Check Your Mouth Campaign is an interactive website designed to help individuals learn to self-discover suspicious tissue changes in their own mouths.
“Early discovery of oral cancers has profound implications. Individuals whose disease is found at early stages of development through opportunistic screenings have less invasive treatments, reducing treatment related morbidity, and there is also the opportunity for better long-term outcomes.”
-Dr. Ross Kerr, Oral Medicine Specialist at NYU
The new website, www.checkyourmouth.org, provides the knowledge and tools needed to recognize and find early symptoms of disease. The process is a very simple visual and tactile process. A person who finds suspect areas in their mouths that persists for over two weeks is then prompted to seek further evaluation from a dental professional.
With a step-by-step video, a very effective and inexpensive intra-oral light from Throat Scope, and examples of abnormalities to look for, this interactive campaign’s objective is to reduce late stage discovery of oral cancer. Throat Scope is available here.

Oral cancer is incredibly deadly, killing one person in America every hour of every day, all year. In 2018, the foundation predicts there will be approximately 51,550 individuals diagnosed with an oral or oropharyngeal cancer.
Of those newly diagnosed today, only about 60% will be alive in 5 years.
To compound the problem, a national screening policy is not in place, and many individuals are not even aware that oral cancer is a significant and increasing common issue in the U.S.
“Reaching the general public with a message can be an expensive idea for a small nonprofit like OCF. Our partner organizations and the members they represent have been long-time leaders of performing oral cancer screenings as a part of the services they provide to patients. These organizations have been champions of routine visual and tactile screenings, and through ongoing advocacy efforts have made them part of the routine screenings dental hygienists perform.”
-Brian Hill, Executive Director of OCF, who is also a survivor of a late stage oral cancer
To help meet that challenge, the Oral Cancer Foundation has engaged two key strategic partners, the American Dental Hygienists’ Association (ADHA) and the Canadian Dental Hygienists Association (CDHA). The combined membership of these partners exceeds 200,000 dental hygienists in the U.S. and Canada.
Now the foundation looks to these long-term partners in screening to introduce their patient populations to the idea of self-exams at home between professional appointments. The foundations should also expose their patient population to the Check Your Mouth concept and website.
Self-examination has become a major part of the general cancer conversation. Other cancer organizations have created campaigns to encourage people to discover abnormalities early. Notable examples are a program to discover deadly melanoma skin cancers early, and self-exams through breast palpation for breast cancers. Check Your Mouth hopes to do the same with their early self discovery campaign.
With the measurable impact of early discovery in other forms of cancer, the Oral Cancer Foundation has moved forward with a similar objective. Oral cancers and their premalignant tissue changes are often easily visible with the naked eye. The model is not so different, with a learning curve that is short and simple to become effective, and an examination process that can be accomplished in about 5 minutes.
The OCF educates and encourages the public to learn the common risk factors mostly found in lifestyle choices such as smoking for oral cancer and avoid them. However, they cannot stop oral cancer from happening.
Clearly, finding the cancer early is the next best idea. Check Your Mouth makes early self discovery easy.
Check Your Mouth is a campaign with the objective of producing better long-term outcomes, which is a very tangible opportunity we can capitalize on today.
Read the original blog by the Oral Cancer Foundation HERE.

For one method of teaching the /r/ sound, I like to use a Throat Scope.
It’s like a glowing tongue depressor from a company called Throat Scope. I absolutely love them!
I’m going to use the Throat Scope in combination with the therapy mirror. It gives the children a really good view of their mouth.
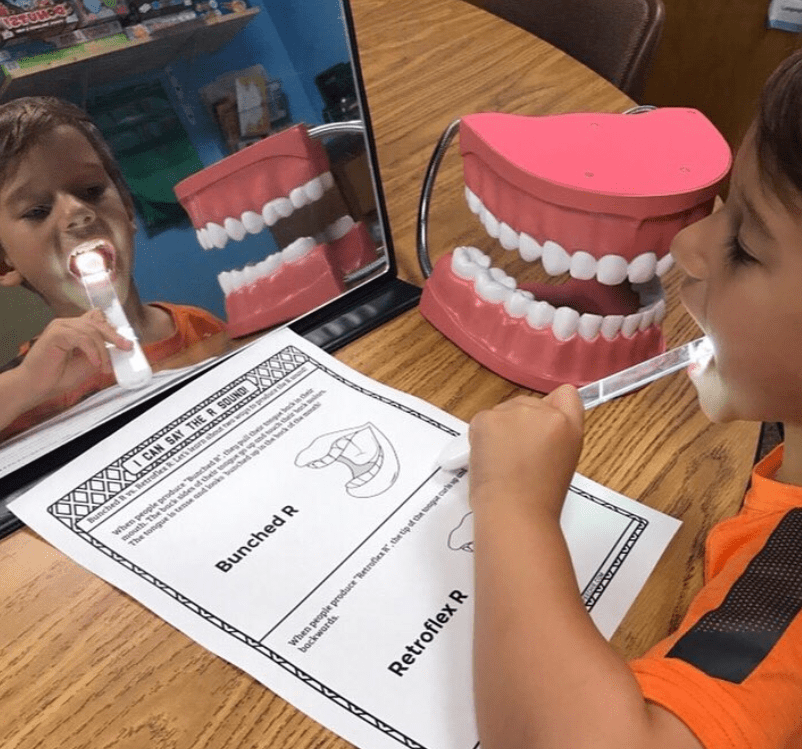
You can really see inside the mouth, and it’s very very bright. That can help them learn anatomy and you can point out the different structures using something like dental swabs.
“See over here? You need these sides of your tongue to go up back here to your back teeth. So say /r/.”
“/r/.”
And they can really see that /r/ sound a lot more clearly.

You can also use a pen light, but I like this because I can actually stick it inside of the mouth, too. So, I could say,
“Okay, right back up here, that’s where I need the sides of your tongue. So put your tongue right back there.”
“/r/.”
And these tips are recyclable. So, when you’re done, you can just recycle them.




Subscribe to get updates on new blogs from Holland Healthcare.

If you’re an SLP and have tried to do some articulation and mirror therapy with a student to help with tongue placement, you’re going to love. this. tool.
It’s called Throat Scope. You can use this to literally light up the inside of a child’s mouth so that they can clearly see where to place their tongue for sounds like /r/, /k/, and /g/.
When I first saw this, I thought it looked kinda like a Darth Vader glowing Light Saber. So, I’m guessing there will be some Star Wars fans out there who think this Scope is pretty cool and would be more than happy to participate! ;)
I’m also thinking about those school nurses and parents who have students with special needs, who have trouble getting kids to open their mouths long enough to see what’s going on in the back of their throat.
At least with Throat Scope, you will get a clear look, even if it’s quick!
It’s simple and easy to use. I found this Throat Scope for about 20 bucks.
I’ve been looking to find some things specifically for SLPs because I so often share ideas that are often more appropriate for special education teachers. I saw today’s tool in a video done by a fellow SLP who goes by the name Peachie Speechie. It’s not only great for when you want to do some mirror work, but it’s also a great tool for parents and nurses!!! I actually ordered this tool online but was hoping to find it somewhere local since the package has a sticker that says, “As seen on TV.”
You won’t want to miss this!

It’s just a light. And this little plastic Saber tongue depressor kind of thing that lights up.
You simply put it into the student’s mouth, and you get a much clearer look.
DISCLAIMER: In this video, it says you “can disinfect blades between students or uses.” HOWEVER, THROAT SCOPE BLADES ARE SINGLE-USE ONLY. Throat Scope blades are FDA-approved for single-use only to eliminate the risk of cross-contamination. Reusing blades puts you and your patient at risk. Please dispose of the recyclable single-use blades in your recycle bin and change blades between each use and each patient.
I’ve been looking to find some things specifically for SLPs, because I so often share ideas that are often more appropriate for special education teachers.
I saw today’s tool in a video done by a fellow SLP who goes by the name Peachie Speechie. It’s not only great for when you want to do some mirror work, but it’s also a great tool for parents and nurses!!! I ordered this tool online.
Read the original blog by Carla Butorac at Behavior Communicates HERE.

Subscribe to get updates on new blogs from Holland Healthcare.

Are you struggling with eliciting the /K/ and /G/ sounds from some of your students or kiddos? Jenna Rayburn from Speech Room News is here to help! Here are 5 tips – okay, more like 7 or 8 tips – to help.
Today we’re talking about the tricky /k/ and /g/ sounds and eliciting /k/ and /g/. I hear a lot of people complaining about those ones.
Let’s talk about Throat Scope. This is something I’ve been using with my /k/ and /g/ kids – actually all my kids – it’s one of those great ‘As Seen On TV’ things! It was made in Australia by a mom. Let me show you what it does.
So it’s a light-up tongue depressor. Watch. Can’t you see my palette, isn’t that awesome?
And it looks like a Light Saber, which makes every kid willing to do it.
What I usually do is a bring a puppet, like a dinosaur puppet, and I have the kiddo do it so they can see what we’re going to do… So then I’m not just attacking them with the light saber.
It’s way better than the cherry-flavored tongue depressors, way better!
I put this in my mouth, and you can see. I don’t have to have a separate pen light.
So for /k/ and /g/, I’ll have it in my mouth… And they make disposable that you can attach. So I’ll have one for myself, and one for the kid, and we can swap out the base. The base is what has the light in it. You put the tongue depressor on and it works. So once you slide the tongue depressor or the blade on there, the light just stays on.
Finally, a therapy tool we can afford!
—
Welcome to the Speechie Show! Being a speech language pathologist often means having too much work and not enough planning time. To beat the overwhelm, we’re bringing you the tricks and tools that will make your job a little bit easier.
Carrie: Hey everybody welcome to the Speechie show. I am your host Carrie Clark with SpeechandLanguageKids.com and I’m here today with Jenna Rayburn with Speech Room News. How are you Jenna.
Jenna: Doing great, how are you?
Carrie: Good, I’m excited to have you on. I know that a lot of my followers also follow you so I’m sure our friends are very excited to see us both sort of in the same place, almost.
Jenna: Simultaneously, kind of. Thanks for having me on.
Carrie: Absolutely. So today we’re talking about the tricky K and G sounds.
Jenna: Da Da Daaa….the dreaded sounds.
Carrie: Absolutely. I hear a lot of people complaining about this one so. Good topic today.
Jenna: And R
Carrie: Yeah, R and K and G and we’ve hit all of those on the Speechie show. If you are new to the Speechie show this is a weekly show where I interview another speech language pathologists and we talk about one topic for a while and we get feedback from you. If you are watching online right now. So, if you are watching with us, what is it..December 5th today…if you are watching with us here on December 5th, go ahead and type in for me in Facebook live. Are you having trouble with the K and G sounds. Or are you good to go, I don’t know why you’re here. But go ahead and if you’re having trouble too, type yes for us so we know you’re here. So, we are going to go ahead and talk about K and G in just a minute. We also have some giveaways coming so don’t skip out. Hang on till the end to get the giveaways. But Jenna why don’t you go ahead and tell us a little bit about yourself for anyone who is not familiar with you.
Jenna: Yeah, well thanks so much for having me on again and we’re going to tackle K and G today. So, my name is Jenna Rayburn and I am a school based speech language pathologist and I live in Ohio. This is my 7th year as a speech therapist and I work in a preschool right now. I’ve done…sorry I have a cold…excuse me….Right now I work in a preschool only special ed program. My district has 13 different elementary schools and then they send all their preschoolers to one building. So, it used to be an elementary school and now it’s a preschool only. So right now, I live preschool all day every day. And about 60% of my week is doing therapy and about 40% of my week is part of the evaluation team. So, every week I do play based assessments for incoming kiddos who are qualified for preschool.
Carrie: That sounds fun.
Jenna: Yeah, and I’ve done up to middle school age. I haven’t really dabbled in the high schooler and beyond but all the pediatric levels I enjoy, but preschool’s my favorite. That’s why I’m talking about K and G because everybody is doing cluster reduction and everybody’s fretting in my land.
Carrie: Absolutely and I don’t see any comments on there. If you all are watching live tell us if you’re working on K and G with any of your students. And you have a giveaway for us too later, what are you giving away?
Jenna: I will be giving away something called Fallen Flakes Finology because I love alliteration. Um and it’s going to have winter activities so you can do those starting now all the way until…if you live in Ohio it snows in April unfortunately…and its all the different chronological processes so you’ll have lots to practice with your students. It’s really interactive so I’ll show you that in a little bit too.
Carrie: Perfect. Ok so everybody hang tight. We are going to be doing giveaways. She’s giving away that. I’m giving away 2 free months in my membership program for speech language pathologists.
Jenna: That’s a good giveaway.
Carrie: Yeah. So, stick around for that. Don’t forget to share this video. The more we share it the more it will go around so if you know someone who needs help with K and G, tag them and share it on their Facebook page. Or share it on your own Facebook page for your friends as well. Alright let’s go ahead and jump in. We have 5 tips to share with you today and Jenna is going to tell us the first one which is using gravity. Jenna tell us about that.
Jenna: Well I guess I’m starting kind of backwards because this is one of my last resort tips, but for some reason I’ve had maybe five or six kids in my career that this was like that one thing that I like well I could’ve done that a month ago, and this would have been a lot easier. But I just use gravity so I usually have them lay on their back or on an exercise ball and we try to use gravity to listen for the “K” or “G” sound, getting that tongue elevated in the back and sometimes no matter how many cheerios I put under their tongue or how many times they hold their tongue tip down, just using that gravity helps them feel it and feel what it’s supposed to feel like. So, it elicits that sound and then we start using strategies when they’re sitting upright because we don’t all just lay on the ground all day. Using gravity sometimes really helps me get that tongue elevated in the back of their mouth.
Carrie: So basically, you’re just having them lay down and having them now say “K”?
Jenna: Yeah, I have them lay on their back and open their mouth as wide as they can and I have them do animal sounds. Which is one of the ways that I elicit it is through animal sounds like having them growling or making a noise like that. So, I have them lay flat on their back and just try to elicit it normally but I’m using gravity to help that tongue get it back there.
Carrie: Ok. So, you could actually, you actually have them lay down and then try other strategies too. So, you could do this with any of them.
Jenna: It’s the last resort.
Carrie: I love it. You know you also mentioned the cheerio thing which I don’t see on our list so will you mention that one? That will be our bonus, you get 6 today guys.
Jenna: Ok six and a half. It’s kind of the same thing I don’t really put in there. But I just always have them hold their tongue tip down with their finger. I don’t try to put my finger in their mouth because I don’t want to get bit #1 and #2, some kids are so gag reflexive…they have an easily triggered gag reflex and I don’t want that to happen so I have then use their own finger and hold the tongue tip down and say that sound “k” Camel. Once I have them do that and I try to wean them off of that I use the cheerio and I have then put a cheerio right underneath their tongue and I have them try to hold down that cheerio with their tongue. Because sometimes if they’re focused on that then sometimes I can get their posterior tongue to elevate so I can get that “k” or “g”.
Carrie: Absolutely. So, that was like three for one guys. We’re banging them out here. Alright so Angela says she always has K and G for her pre-k kiddos definitely. So, and looks like Frahannah just shared the video, thanks. So, don’t forget to share the video guys and stay tuned cause we’re doing some giveaways.
Jenna: Yeah
Carrie: Also, if you guys have any questions about eliciting K and G or any of the strategies we’re talking about right now, go ahead and type those in. If you are watching with us live, we’ll answer them now. If you are watching later then we’ll answer them whenever we can get back to you. So alright let’s move on to #2 slash 4…hahaha…wherever we are. So, that one is utilizing animal sounds. Tell us about that one.
Jenna: So, preschoolers have such a hard time following a one stop direction like “throw this in the trash can” and if I try to give them a one-step direction that relates to their mouth and lifting their tongue, it’s just too hard. So, I always start with that natural, however I can elicit that sound that they might already be doing through animal noises or car noises or train noises or whatever it’s called. And so, I usually use animal noises like a growling sound to elicit that “grr” sound in the back. And sometimes even if they’re not doing it at all in any place in words, I’ll hear it in that animal sound. So, that’s kind of like the first thing I ask them to do if I’m going to check for sounding ability or check if they can even do it. Before I even say ya know “watch my tongue and copy what I do” I just say “oh let’s pretend we’re bears grrrr” and I just try all these different sounds and see if I can elicit it though an animal sound.
Carrie: Yeah, I’ve also done like kind of a monster sound so we’ll just go like krrrr. Which it’s kind of like a stretched-out K almost and that seems to help for some of my kids and they really have fun with that too.
Jenna: Yeah, to get that voiceless sound. And then my next tip kind of falls back so then for the “k” I usually do the cough sound. I’m like “oh let’s fake a cough” k…k….k…and I like mold their cough into a K cough.
Carrie: Yeah. Ok if you guys have used one of the animal sounds or coughing, lets type in what you call that. So, like what kind of sounds, is it a monster sound. What’s worked for you, for your kids. And then touching on that I’ve noticed once you can get them to make like a coughing sound or like a “K” kind of growling sound the you can kind of like you said, shape it down so you can say ok let’s practice on making that really short. Or really choppy and try to get them to do it different ways that sounds more like a K without actually telling them their making the K. Because them of course they’re like oh yeah Tah Tah that’s my K.
Jenna: Yeah, I guess that should have been my very first step and that’s what I always do is I rename the sound. So, if it, whatever is the trigger that helps like if you’re lying on your back and you get it, I’ll call it your napping sound.
Carrie: Nice
Jenna: Because you were laying on your back when you got it. If you were growling like a bear when you got your “gah” it becomes the bear sound. Now if you walked into private speech therapy and said I’m working on my bear sound, that person might not know, but that doesn’t matter cause to me I’m just trying to help that kiddo reframe that. Because you’re right, the first time you say ok now practice Kah sound he’s going to go t t t.
Carrie: Yeah, we don’t talk about the K sound.
Jenna: And sometimes I call it a new sound if I can’t get the kid to elicit it, like if nothing worked right off the bat, I just call it your new sound… “oh let’s do that new sound that we practiced last week”. So, it becomes the new sound. Anything but calling it the K or the G sound.
Carrie: Yeah and Shannon is saying they call it the back sound, so that’s good too, I like that. Yeah and then of course you’re going to call it by what it is once they can do it, but you have to break that mindset first.
Jenna: Yeah
Carrie: Definitely. Alright.
Jenna: To change that pattern.
Carrie: Uh Ha, absolutely. We have a ton of people on here. We have 26 people live on here watching right now. Thank you, guys, for joining us. Don’t forget to share and stay, stick around because we’re going to do some giveaways here in just a sec. We have two more tips for you. We’ve already thrown out a huge number of tips so far. So, let’s do Hippo mouth. Tell us about hippo mouth.
Jenna: Hippo mouth. I use to just call it the open mouth but then one of my kiddos was like “it’s like a hippo mouth” because when you think about a hippo mouth they open their mouth so wide that’s like the biggest mouth I can think of so now I use the hippo mouth.
Carrie: I like it.
Jenna: So now when all else fails I just tell the kiddos to open their mouth as wide as then can like the widest. Everyone do it with me. If you have your mouth open as wide as you can, you cannot say tah. Ya just can’t make a T instead of a K.
Carrie: Nope
Jenna: Now you might not be able to get a good K, but if you have your mouth open as wide as you can you can kind of shape it from there because you just can’t make a tah when your mouth is open as wide as you possible can.
Carrie: Perfect, I love that one. Yeah, the first time I tried that and it worked with a kid I was like are you kidding me, I just needed to tell you to open your mouth…hahaha
Jenna: A hippo mouth? Ok great we’ll do this forever! So just opening your mouth as wide as you can, you really can’t. And as I start bringing it back down I start doing that finger hold kind of thing to keep that tongue down. But we just practice it with our mouth wide open as we can. We’ve got out hippo mouth.
Carrie: Awesome, I love it. I love it. Let’s see Mel, thanks for joining us Mel. Ok we have one more tip to share with you. If you’ve missed any of the tips leading up to now we’ve, you will be able to watch the recording afterwards, but we have one more tip to share and then we’ll be moving into our giveaways so stick around. Mel says the hippo sounds fabulous. Absolutely I agree…hahaha. Ok so our last one is, when all else fails, cycle. Tell us about that.
Jenna: Cycle it. I think that K and G is one of those sounds that you could like bang your head against the wall everyday if you have a kid who just can’t get it. I’ve only had one kid I sent to Kindergarten that never ever got it and she had autism and so I, theirs other kids out there. But if you cannot get it, there is no point in practicing it wrong a hundred times a day if you don’t have other things to work on. I just don’t think it’s worth it. So, what I do if I have a kid who I cannot get um it in in any place. I can’t get it in isolation, we’re not even close, I just kind of put it aside. Even if I think theirs other, if that target is more important than other ones and I use the cycles approach and I cycle it. So, we’ll work on it and we might do auditory the whole time but we’ll work on it for a little bit, do auditory, work on the elicitation and then put it away for a few weeks. And sometimes it’s hard to do the cycles in a school setting. It’s hard for me too, so I just try to run through it so that I’m making sure I put it, you know I kind of think about it in months at a time. So, this month we’re really going to work on it and then I’m going to put it away and then I might test it again and see if we’re ready to try it again at a later date.
Carrie: How often do you cycle back? Does it depend on how many goals they have?
Jenna: Most of my kids have goals for like two to three processes. So, that could be a lot of cycle because we’re writing yearlong goals. So, that could be a lot of cycles when you think about your breaking it down to like the individual sounds within those processes and if you’re thinking about blends and taking those apart. So, when you’re thinking about that, there is a lot to be targeted. So usually I have plenty to work on if I can’t get the K and G and I’ll just come back to it and I’ll keep coming back to it and make sure the kiddo is still aware of it. Still going to do auditory but just naturally when I’m doing therapy on other things but I definitely cycle through it. Just try not to beat your head against the wall with it if you can help it.
Carrie: Yeah
Jenna: It frustrates the kiddo too cause it’s hard to have your speech therapist everyday to say you’re not doing it right and you want to find success.
Carrie: Yeah, I’ve found that the months seems to be a pretty good time frame in terms if you’re going to try something and not making any progress in a month, especially in the schools, that seems to be a pretty good like “ok we gave it a good month, let’s put that one away and come back to it”. So, I agree.
Jenna: I see my kiddos twice a week so that would be like 8 different sessions so I thinks that’s a pretty fair amount of time. If I haven’t been able to get it at all then I’ll just put it on the shelf and then take a month off and then try it again.
Carrie: Absolutely. Alright we have a couple comments here.
Angela says “I always say use your cough sound”. Have them cough into their elbow when producing it. Hopefully help them to cover their mouth when they really are coughing…hahaha…yep.
Debbie is watching from Kuwait, wow welcome you get the furthest person away award. And
Chelsie says I call the G gulping water and the K knocking door sound.
I like that, those are good names.
Jenna: I may have to steal that.
Carrie: Ok perfect. Alright we have reached the giveaway stage so if you guys are watching on Facebook live with us right now on December 5th you are eligible to enter the giveaways. I have to preface this. I’ve had some people try to enter via email and that’s not how this works so I’m going to give this analogy. So, it’s like watching Jeopardy at home and shouting out your answer, you don’t get to win. So ya have to be in our live studio audience which happens to be on Facebook right now. Ok so for giveaways talk about what you’re giving away and any other resources that you like for K and G.
Jenna: Yeah so first I’ll talk about a hard resource I’m holding it. So, this is a product that I have been using like crazy with my K and G kids. Actually, all my kids, but let me hold up the box so you can see it. If you just screenshot it, this would be a good time to do that so you can see what it is. I’ll throw a like in here when we’re done being live. But it’s one of those great “as seen on TV” kind of things that was made in Australia by a mom and let me show you what it does. So, it’s a light up tongue depressor…watch…
Carrie: Oh, my gosh that is so cool.
Jenna: Can you see my pallet? Isn’t that awesome. Also, it looks like a lightsaber which makes every kid willing to do it. What I usually do is bring a puppet. I have a dinosaur puppet and I have the kiddo put it in the puppets mouth so they can see what we’re going to do cause then I’m not just like attacking them with the light saber. And then it’s way better than the cherry flavored tongue depressors.
Carrie: Hahahaha…absolutely.
Jenna: You have them put this and then you don’t have to have a separate pin light, its way better. So, for K and G I’ll have it in my mouth and they make disposable blades that you attach. Here’s like one of the blades. So, I’ll have one for myself and one for the kid and we can swap out the base. The base has the light in it when you put the tongue depressor on it, it works.
Carrie: That’s awesome!
Jenna: I know right! So, once you slide the tongue depressor or the blade on there it just stays on.
Carrie: I love it!
Jenna: Alright so it’s called Throat Scope. It was made in Australia but it’s available in the US as of January, so perfect timing and it’s like $15 or something.
Carrie: Woah!
Jenna: Finally, a therapy tool we can afford!
Carrie: Right! Yeah Emily says she wants that. I agree, I want it too.
Jenna: I think it’s throatscope.com I’m pretty sure and you can preorder them. I’m going to order like a bunch because I need one in my bag and my rolling cart. I’ve had mine since the beginning of the school year and I’ve been using it like crazy. And then they sell, the package comes with like your Throat Scope, the base and then three blades for like the $15-18, whatever the price was and then you buy the replacements in bulk. Like doctors, therapists, those people.
Carrie: Nice
Jenna: Yeah so, it’s still pretty cheap it’s like $20 bucks for a big thing of blades and it’s lasted me. I haven’t run out yet this year. So, that’s called the Throat Scope and that’s my first favorite tool.
Read the original blog from Speech and Language Kids here.
Subscribe to get updates on new blogs from Holland Healthcare.

Have you heard of these things called Throat Scope? No? Well then my friend prepared to be wowed! Yes, wowed by something that you use to look in someone’s mouth. As SLPs, we tend to appreciate these innovations more than others, that is why Throat Scope is something I just couldn’t wait to share. It is an absolute game changer for oral mech exams.
 How many times have you done oral mech exams? 20, 50, 100, maybe more?! Then you know the drill: pop in the tongue depressor, hope that the battery in you light you have been using hasn’t died, and if it still works, take a look around. Not a big deal, but it is a necessary step in the screening and eval process.
How many times have you done oral mech exams? 20, 50, 100, maybe more?! Then you know the drill: pop in the tongue depressor, hope that the battery in you light you have been using hasn’t died, and if it still works, take a look around. Not a big deal, but it is a necessary step in the screening and eval process.
Well, this step just got a whole lot cooler! Throat Scope is a light up, clear tongue depressor that allows you a much better view of oral cavity without testing your ability to juggle a flashlight and depressor while not shining the light in your student’s eyes as well.

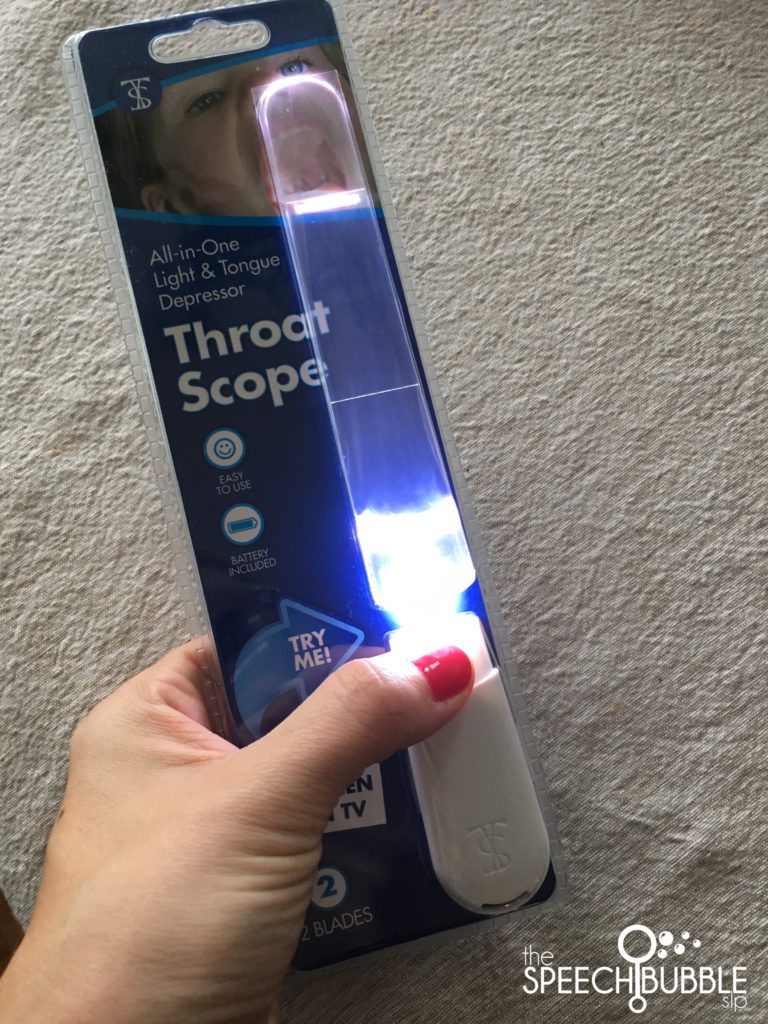
Here is the Throat Scope. It kind of looks like a speechie light saber. You can use your SLP Jedi powers and do a killer oral mech exam.
Yup, each time. You wouldn’t believe how many students I have had that ended up having an physical reason for their speech that would have gone (or had already gone) overlooked! If I hadn’t taken the few minutes to do a quick look around I would have missed tongue ties, submucousal clefts, huge adenoids, crazy high arches palates, etc. These issues and more had contributing factors that needed outside attention in order for those kids to make progress.
You just pop on a new blade aka clear tongue depressor, and it automatically lights up. I liked not having to hold down a button while using it. This also means that you don’t have to worry about not turning it off and running down the battery (like I have done with all mini lights and secret message decoder lights from Super Duper).

The light is nice and bright so you can really see everything. This is such a step up from trying to mange the old wooden tongue depressors and flashlight combo. A total upgrade. Another win for Throat Scope, they don’t break the bank! You can get the light and 100 replacement blades, because you are only using one per kid of course (they’re recyclable), for $45! That is pretty darn good if you ask me. Yes, they might be a bit more than the wooden tongue depressors but think of 1) how many oral exam you really do in a year and 2) how much more efficient these are.
Read the original article byMaureen Wilson at The Speech Bubble SLP HERE.
Subscribe to get updates on new blogs from Holland Healthcare.