What are people saying about Throat Scope? Pediatricians, general practitioners, primary care physicians, dentists, speech-language pathologists and more across 155 countries are using Throat Scope. Read reviews from professionals across all scopes of practice.
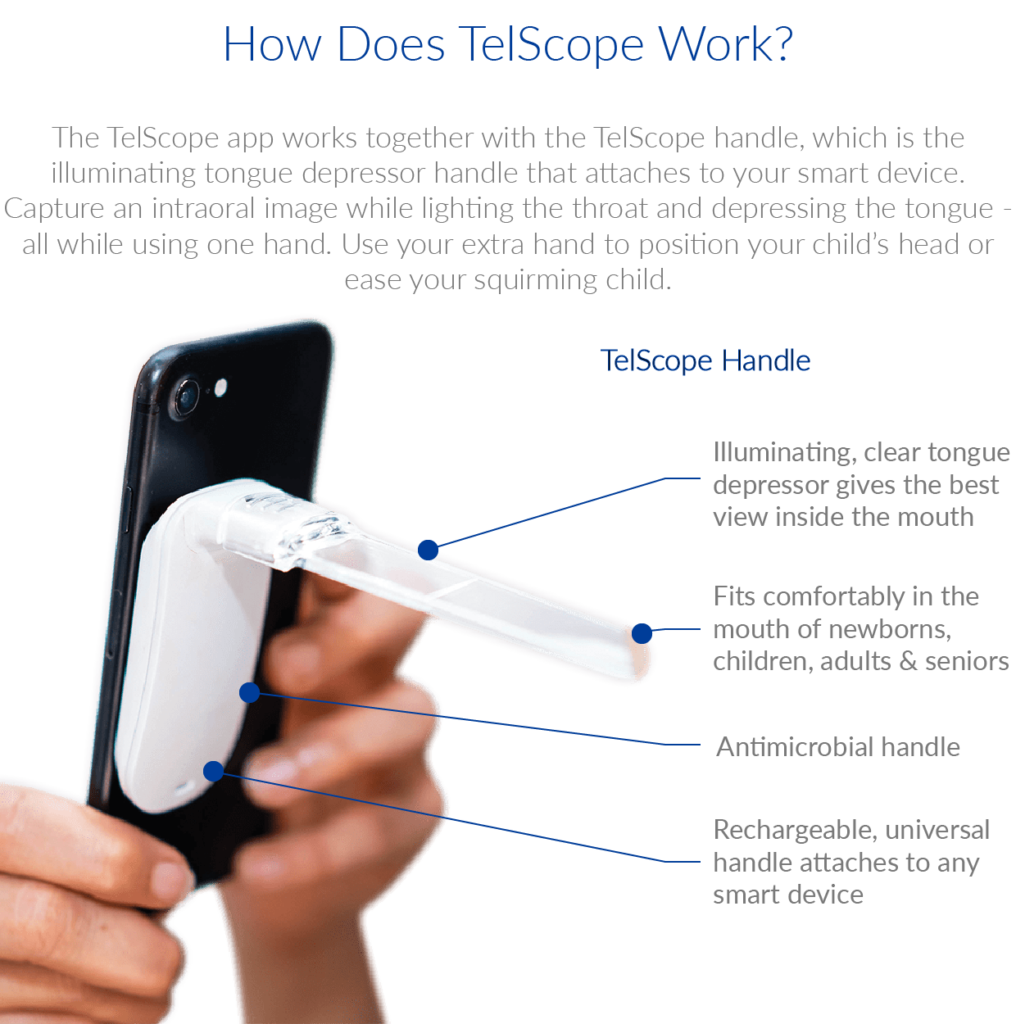
Throat Scope makes experiences for yourself and your patient faster, easier, and most importantly – more accurate. Throat Scope frees up an extra hand instead of the old flashlight-depressor combo by placing the light source directly inside the mouth.
Throat Scope is also used as a speech and articulation tool, an examination tool, and an oral cancer screening tool.

Here’s what people are saying about Throat Scope:
“This is an absolute essential for every dental and medical practitioner to provide the best possible oral assessment and ability to discover oral cancer in its earliest stages.”
Jo-Anne Jones – Dental Hygienist & Oral Cancer Motivational Speaker
:This is a product that I have been using like crazy with a few of my /k/ and /g/ kids, actually all of my kids. It also looks like a light saber which makes every kid want to do it. Finally a therapy tool we can afford!”
Jenna – Speech Language Pathologist – Speech Room News
“I’m a school nurse and with all the strep and flu going around, I am going to fly through my box of 100!
Throat Scope is life changing for me! It makes checking kids a breeze. I am awestruck! I’m a “one man band” it’s singing praises to professionals and family and friends. Brilliant!”
Paula – School Nurse
“We are loving using our new Throat Scopes in the clinic. What a difference it makes to be able to see inside our ‘littlies’ mouths quickly and easily. What a great idea! Also very useful for identifying air escaping down the nose during speech for our Cleft Palate clients as it so happens!”
Kim – Speech Language Pathologist
“Throat Scope is high-tech compared to the organic incumbent.”
ZD Net – Worldwide News Media
“Throat Scope provides medical professionals with one free hand, a light source located inside the mouth for a fast, accurate and pleasant oral examination experience.”
The Daily Floss Worldwide News Media
“One word: Genius.“
SLP Toolkit – Speech Language Pathologist
“It lights up the whole mouth! You can see a lot more than redness at the back of the mouth #brilliant“
Eva Grayzel – Motivational Speaker for Oral Cancer
“Parents and school nurses who have students with special needs who have trouble getting their kids open their mouths long enough to see what going in the back of their throat. At least with Throat Scope, you get a clear look even if it is quick!”
Carla Butorac – Speech Language Therapist
“This award comes with a lot of “firsts”. While only a couple of Australian companies have been honoured with an Edison Award since their inception in 1987, Holland Healthcare is the first Australian female led company to be recognised. It is also the first Australian medical device to win.”
Hunter Headline Newcastle Newspaper
“Cannot believe my daughter did not gag. She was so excited to have Throat Scope that she didn’t mind the usual discomfort that goes along with an oral examination!”
Katy – Speech Pathology Mama
“No more juggling with a torch and a wooden craft stick to look into a kid’s gob. It’s a blessing for clinicians and parents. Who knew oral cavity examinations could be so much fun?”
The Australian Newspaper
“The Throat Scope is great. More kid friendly than a traditional tongue depressor and pen-torch, for assessing children’s mouth and throat.”
Kathryn Harber – Speech Language Pathologist
“This product is well made and arrived really quickly. I love the product and it’s been very useful already.”
Melody Humphries- Speech Language Pathologist
“It works, reduces the materials I need, and engages kids. It’s a win.”
Jenna – Speech Language Pathologist – Speech Room News
“Having another ‘tool’ to help illuminate challenging areas of the mouth including the tongue, floor of the mouth, palate and throat makes earlier discovery more feasible. Great adjunct for screening examinations and oral self exams.”
Jo-Anne Jones – Motivational Speaker on Oral Cancer
“This is an SLP’s dream!”
Amanda Schaumburg – Speech Language Pathologist – Panda Speech
“My kids love it, it has a light saber element to it.”
Nacole – Registered Nurse – NurseNacole
“I have 3 of these scopes, one in each exam room. I purchased 150 count of the blades. I use them not only in assessment but in treatment with patients. I place one blade with each patient for sensory targets, or useful in resistive exercises and in demonstrations of therapeutic exercises-side by side.
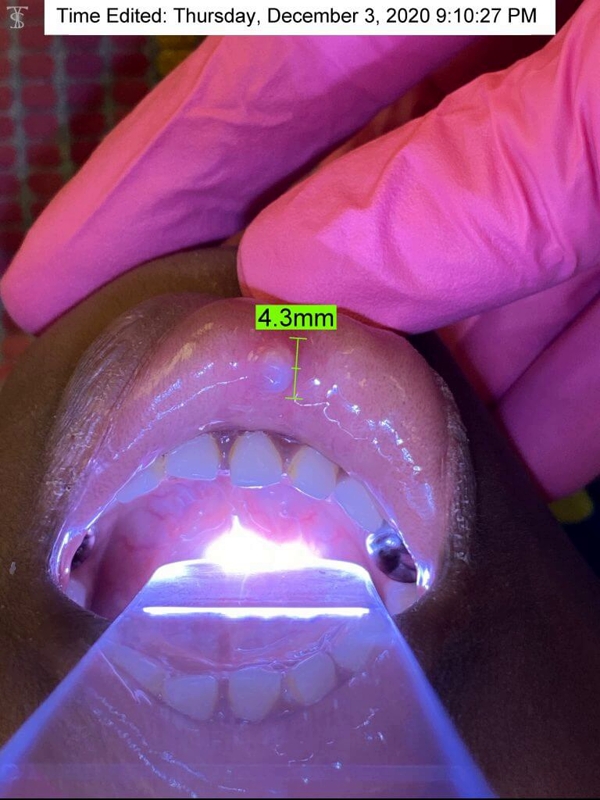
I also use these with my current cancer patients undergoing radiation treatment . I am able to take photographic images for communication with the radio-oncologist and or ENT to quickly manage mucositis; thrush and lesion development.”
Tamatha Rutherford – Speech Language Pathologist
“This is a great product especially for patients with structural abnormalities, oral apraxia or macroglossia which can make visualizing the oral cavity a real challenge! Much more effective than using tongue depressor in one hand and pen light in the other!“
Anne Brockman – Speech Language Pathologist
“Throat Scope is a game changer for OME and oral exams”
Graham Speech Therapy – Speech Language Pathologist
“Best Intraoral Exam Tool Ever.“
Dr Keith Grimes – UK Doctor
“My area of specialization in dermatology is blistering diseases. Patients may have erosions and blisters inside the mouth as well as other mucous membranes and of course, on the skin. During these patient reviews, I have found it time saving and patient friendly to wear the lanyard which attaches to a device called a ‘throat scope’ which contains a battery-powered light. There is a disposable see-through plastic tongue depressor which is individually wrapped that I attach to this in order to easily view inside the mouth and take photos with my free hand. It is also useful for examining the mouth for skin cancers and infections.”
Dedee F. Murrell, Professor of Dermatology, University of Sydney, Australia
“I could be a salesperson for Throat Scope. I love this tool and use it daily as a clinician . As a clinical teacher, I’m constantly introducing it to the next generation of SLPs. Not only is it functional, but it is also fun. A” must have ” when working with pediatrics.”
“Received my delivery today (arrived within days of placing my order). Had a little play around and am very impressed with the quality of manufacture and ease of use. What a valuable tool to have at home and very affordable. I hope to see my GP using this next time I have to visit.”
“Just received this, and with frequent mouth ulcers I expect it will help. BUT, I ordered a 2nd set for my neighbor who has 15 grandkids, the oldest being 16 yrs old, and the youngest being 2 yrs, 1 yr, and 3 days old. Giving it to her since most of the kids are in and out of her house every single day. Thanks for a simple but genius product!“
“Great product! So useful for dental assessments particularly when assessing clients outside the dental clinic. (ie. in ages care facilities) and apprehensive children.”
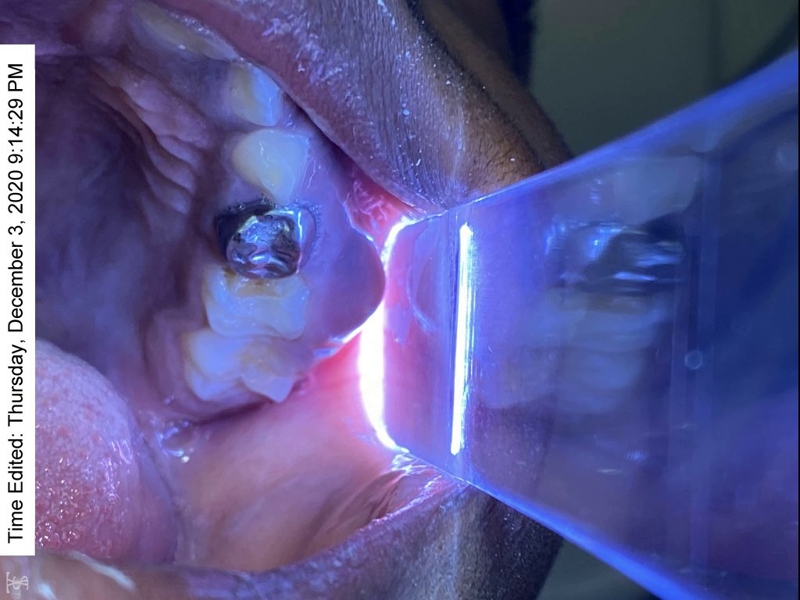
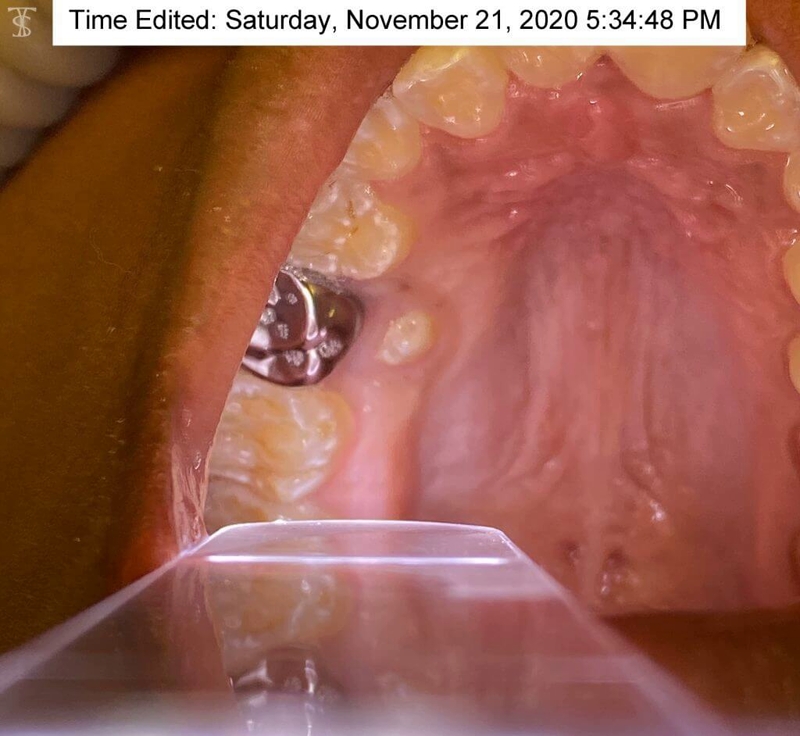
“I love this product – I love this product, all the oral cavity can be seen and even deep into the pharyngeal walls. The light is bright enough and the scope is clear to allow a better view. The throat scope is easy to use, once you connect the clear tongue depressor to the white attachment the light turns on and it’s ready to use. Clear disposable plastics are available and can be placed on the clear tongue depressor for each person.”
“A must have for every SLP! I am a speech-language pathologist and Throat Scope is so helpful for my job! This makes completing oral mech exams so much easier!”
“Came as pictured, words great, very fast. This came exactly as pictured and very quickly! It was super helpful checking my kids after tonsillectomies for healing process and at work for oral mech exams.”
“Good for moms to check their kids throats.”
“These work great. Take it from the Doc, these are worth the cost.”
“Effective to detect problems in the throat. These are very useful when my children get sick.”
“FANTASTIC! This a great product and it performs exactly as advertised. It makes it real easy to see in the persons mouth. I highly recommend it.”
“Great tool! This is an awesome invention. Completing an oral assessment or checking your kids throats or teeth- light and tongue blade in one hand!!!”
“Great product, I even bought one for my doctor!”
“Useful and affordable.”
“I cannot wait to use these in the upcoming school year. This product will make oral examinations much easier than holding a flashlight in one hand and a tongue depressor in the other.”


































 My brother was in town and I forced him to let me inspect his oral cavity using the throat scope. I was surprised at the amount of light the Throat Scope puts out. It definitely works!
My brother was in town and I forced him to let me inspect his oral cavity using the throat scope. I was surprised at the amount of light the Throat Scope puts out. It definitely works!